Escoliose e cifose
Curvature of the spine
Revisado por Dr Hayley Willacy, FRCGP Última atualização por Dr Colin Tidy, MRCGPÚltima atualização 16 Mar 2023
Atende aos diretrizes editoriais
- BaixarBaixar
- Compartilhar
- Language
- Discussão
- Versão em Áudio
- Adicionar às fontes preferidas no Google
A escoliose é uma condição nas costas que faz com que a coluna vertebral (das costas) se curve para o lado - seja para a esquerda ou para a direita. A maioria dos casos se desenvolve em crianças entre 9 e 14 anos durante o surto de crescimento da puberdade. A escoliose geralmente é leve e não necessita de tratamento. Para casos mais graves, os tratamentos incluem exercícios específicos, um colete ortopédico ou, ocasionalmente, cirurgia para endireitar a coluna. Uma curva muito acentuada de frente para trás é chamada de cifose, que geralmente não necessita de tratamento.
Em resumo
Scoliosis is a sideways curve of the spine.
A curvatura pode ser leve ou grave, e em diferentes partes da coluna.
A maioria dos casos de escoliose não tem causa conhecida e frequentemente aparece durante a puberdade.
Os sintomas podem incluir uma protuberância nas costas ao se curvar ou ombros/quadris desalinhados.
Monitoramento regular, fisioterapia, um colete ortopédico ou cirurgia podem ser opções de tratamento.
What is scoliosis?
Escoliose
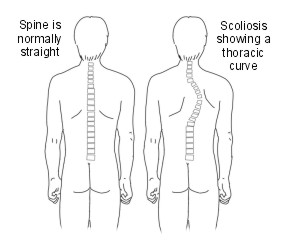
The word scoliosis comes from the Greek word meaning crooked. The back (spine) should look straight, up and down, when you look at someone from behind. If the spine has a sideways curve, it is called a scoliosis.
The curve can bend to the left or to the right. The severity of the curve can vary from very mild and barely noticeable to severe.
The curve can be in the lower part of the spine (a lumbar curve), in the upper part of the spine (a thoracic curve) or go from the upper to lower part of the spine (a thoracolumbar curve). In some cases there is a double curve - like an S shape.
What is the difference between scoliosis and kyphosis?
If you look at someone from the side, normally there are three slight front-to-back curves in the spine - one in the neck, one in the chest section and one in the lower back. An abnormal, more pronounced front-to-back curve is called a kyphosis. This is different to a scoliosis which isn't noticeable from the side.
What are the causes of kyphosis?
Kyphosis can occur at any age, although it is rare at birth. Adolescent kyphosis, is known as Scheuermann's disease.This type of kyphosis is caused by the wedging together in a row of several bones (vertebrae) of the back (spine). The cause of Scheuermann's disease is unknown.
In adults, various conditions affecting the spine can cause a higher risk of kyphosis, including:
Artrite of the spine.
'Afinamento' dos ossos (osteoporose) of the spine, if it has caused one or more of the bones in the spine to flatten (called a wedge-shaped fracture).
The treatment usually depends on the underlying cause. This is covered in the separate leaflets on those specific subjects - follow links in red.
What causes scoliosis?
There are several different types of scoliosis and the causes of each are different:
Non-structural scoliosis (functional or postural scoliosis)
In this type, the back (spine) is structurally normal, but looks curved because of another condition such as having one leg that is significantly longer than the other or muscle spasm in the back muscles. The curve is usually mild and it changes or goes away when the person bends sideways or forwards.
Structural scoliosis
In these cases, the curve is fixed and doesn't go away when the person changes position. There are different types:
Idiopático. This means the cause is not known. For more than 8 out of every 10 people with scoliosis the cause is idiopathic.
Neuromuscular scoliosis. This means the curve is caused by a condition which affects muscles or nerves of the back. For example, it may happen in some people with distrofia muscular, exigências de vacina contra a poliomielite, paralisia cerebral, or neurofibromatosis. Each of these conditions has other symptoms and problems in addition to a scoliosis. In around 1 out of every 10 people with scoliosis it is due to a neuromuscular problem.
Osteopathic. This means as a result of a bone abnormality.
Congenital scoliosis. This means the spine has not formed properly while the person was a baby developing in the womb. Around 1 in every 10 people with scoliosis have had it since birth.
The rest of this leaflet is about the most common type - idiopathic scoliosis.
Who develops idiopathic scoliosis?
Idiopathic scoliosis can develop at any stage in childhood. It is not known how or why it develops. It is confiar due to poor posture and you cannot prevent it starting.
It most commonly develops during the growth spurt of puberty and early adolescence. This is usually between the ages of 10-12 years for girls and 11-16 years for boys. About 1 in 40 children have some degree of scoliosis. Mild scoliosis affects about the same number of boys and girls. However, moderate or severe scoliosis is more common in girls.
Idiopathic scoliosis is not a straightforward hereditary condition. However, about 1 out of every 4 people affected with scoliosis have one or more other family members with the same condition.
Idiopathic scoliosis symptoms
In most cases the onset of the scoliosis is gradual and painless. Scoliosis is usually noticeable on bending down. Sometimes a mild-to-moderate scoliosis can develop without being noticed by the child or their parent/s. This is often because the condition usually develops during adolescence when children often become more self-conscious. Parents and others are less likely then to see a naked back (spine) and see the problem.
Scoliosis can cause mild pain and imbalance of the muscles. If scoliosis becomes more severe then it can become more disfiguring. This is because when the spine curves sideways, as the curve becomes more severe, the small bones (vertebrae) that make up the spine also twist around. This pulls any attached muscles, ligaments and ribs around with them. As a consequence:
If the scoliosis is in the chest (thoracic) region, the ribs and shoulder blades stick out like a bulge on one side of the back. Also, one shoulder may hang lower than the other and one shoulder blade may be higher than the other.
If the scoliosis is in the lower back (lumbar) region, it can make the pelvis thrust forward on one side and one leg may appear to be shorter than the other.
If scoliosis is not treated and becomes severe, it can cause problems later in life. For example, persistent back pain may develop and it can affect your general fitness and your overall quality of life. If the deformity is very severe, breathing problems or heart problems may develop - this is fortunately rare.
If a child has back pain it is very unlikely that it is due to scoliosis. For more common causes of children's back pain, see the separate leaflet called Back Pain in Children.
How is idiopathic scoliosis diagnosed?
Scoliosis diagnosis
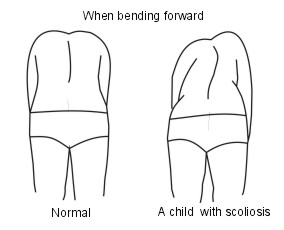
Scoliosis is often seen when you bend forward. A bulge on the back (spine) is more obvious when bending forward.
If your doctor diagnoses scoliosis then you will usually be referred to a specialist.
X-ray pictures of the back are sometimes done to assess the angle of the curve. This gives an idea of the severity of the condition and the likelihood of it getting worse. Other investigations - for example, magnetic resonance imaging (MRI) scanning ou computerised tomography (CT) scanning of the neck - are needed in some cases.
What is the treatment for idiopathic scoliosis?
The aims of treating scoliosis are:
To prevent the curve becoming worse.
To avoid the need for surgery in later life.
To prevent breathing problems.
To improve how the spine looks.
People with more severe scoliosis may need treatment to stabilise the back (spine). Many people with scoliosis do not need treatment.
Treatment depends on various factors, such as:
The person's age.
Whether they are female or male - scoliosis in girls tends to worsen more quickly.
Whether they are still growing.
The severity of the curve.
The exact location of the scoliosis - for example, the upper (thoracic) or lower (lumbar) back.
The chance that scoliosis may progress.
Treatment options include observation, specific physiotherapy exercises, wearing a brace, and surgery. The international Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) recommend that non-surgical treatment should be delivered by a specialist team to include a doctor, physiotherapist, orthotist and possibly also a psychologist.
Observação
Most people have mild scoliosis and do not need any treatment. However, a specialist may arrange regular reviews to make sure that the scoliosis is not getting worse as children get older. Once the main bone growth ends after puberty, scoliosis does not usually worsen.
Sports and other activities can be done normally - there is some evidence that sport and exercise make people with scoliosis feel better about themselves and that they have fewer emotional problems. Occasionally, a specialist may advise against certain activities such as heavy contact sports or gymnastics.
Fisioterapia
Research that shows that specific exercises help to prevent scoliosis worsening has recently been published. The exercises are called physiotherapeutic scoliosis specific exercises (PSSE) and need to be performed from twice a week to daily and occasionally several times a day. This requires a lot of motivation.
Back braces
There are several different types of back brace. The more modern ones are more comfortable to wear than the older ones. If the scoliosis is moderate or becoming worse, then a back brace may be advised, either alone or in addition to PSSE. A brace does not cure a scoliosis. The aim of a brace is to prevent the scoliosis from becoming worse as the child grows. A brace is worn most of the day and night.
Towards the end of treatment they often only need to be worn at night. Most normal activities can be done whilst wearing a back brace. However, they need to be removed for washing and swimming. Wearing a back brace can be difficult for a young person to stick to. An expert team will involve them in the decision to wear a brace, so that they understand why they are doing it and what they are going to gain from it - if it isn't worn, it won't work.
Cirurgia
An operation is sometimes advised for people with severe scoliosis, although if a brace is worn it should be possible to prevent the need for surgery. The aim of the operation is to correct the curve, to stabilise the spine and also to fuse the curve. Spinal fusion is the joining of two or more back bones (vertebrae). Implants or rods are often used to keep the back straight after the operation. These rods are usually lengthened every 4-6 months as you grow.
There are different surgical techniques used. Your specialist will be able to advise which type of surgery, if any, may be beneficial for you. In general, the operations done for scoliosis are usually very long procedures and involve many months of recovery afterwards. Also, they are not always successful.
Tratamentos alternativos
There is good-quality research that has shown that osteopathy does not help to resolve or improve scoliosis. There is also no reliable evidence that other techniques, such as chiropractic, reflexology, acupuncture, neurostimulation, are effective. However, some people with scoliosis find one or more of these complementary therapies to be useful to improve backache or pain.
Escolhas do paciente para Distúrbios do pescoço e coluna

Ossos, articulações e músculos
Dor nas costas e coluna
Dores nas costas são extremamente comuns; a maioria de nós terá dor nas costas em algum momento. Crianças podem ter dor nas costas, mas é mais comum em adultos. Este folheto fornece algumas informações gerais sobre as costas e a dor nas costas. Também irá direcioná-lo para páginas com informações mais detalhadas sobre as diferentes condições que podem causar dor nas costas.
por Dr. Toni Hazell, MRCGP

Ossos, articulações e músculos
Problemas nos discos da coluna
Os discos espinhais também são chamados de discos intervertebrais. Há um disco espinhal entre cada osso (vértebra) na sua coluna. Isso mantém as vértebras separadas e atua como um amortecedor. À medida que envelhecemos, os discos espinhais gradualmente se danificam e isso pode causar problemas como dor nas costas. Outros problemas que afetam os discos espinhais incluem um disco deslocado ou, muito mais raramente, infecção (discite).
por Dra. Hayley Willacy, FRCGP
Perguntas frequentes
Can poor posture cause scoliosis?
Não, a escoliose idiopática, o tipo mais comum, não é causada por má postura. Também não pode ser prevenida melhorando conscientemente a postura.
É normal a escoliose causar dor?
A escoliose geralmente começa de forma gradual e indolor. Embora possa causar dor leve e desequilíbrio muscular, é muito improvável que a dor nas costas em crianças seja causada por escoliose. Se a condição se tornar grave, a dor nas costas persistente pode se desenvolver mais tarde na vida.
Quão comum é a escoliose idiopática em crianças?
Cerca de 1 em cada 40 crianças tem algum grau de escoliose. A escoliose leve afeta meninos e meninas igualmente, mas casos moderados ou graves são mais comuns em meninas.
Existem terapias alternativas que podem curar ou melhorar a escoliose?
Pesquisas mostraram que a osteopatia não ajuda a resolver ou melhorar a escoliose. Também não há evidências confiáveis de que outras técnicas como quiropraxia, reflexologia, acupuntura ou neuroestimulação sejam eficazes no tratamento da condição em si. No entanto, algumas pessoas acham essas terapias complementares úteis para gerenciar dores nas costas ou dores associadas à escoliose.
Minha escoliose vai piorar após a puberdade?
Para a maioria das pessoas, uma vez que o crescimento ósseo principal termina após a puberdade, a escoliose idiopática geralmente não piora.
Leitura adicional e referências
- Monticone M, Ambrosini E, Cazzaniga D, et al; Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. Eur Spine J. 2014 Jun;23(6):1204-14. doi: 10.1007/s00586-014-3241-y. Epub 2014 Feb 28.
- Theis J, Gerdhem P, Abbott A; Quality of life outcomes in surgically treated adult scoliosis patients: a systematic review. Eur Spine J. 2014 Nov 8.
- Negrini S, Minozzi S, Bettany-Saltikov J, et al; Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst Rev. 2015 Jun 18;(6):CD006850. doi: 10.1002/14651858.CD006850.pub3.
- Negrini S, Donzelli S, Aulisa AG, et al; 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi: 10.1186/s13013-017-0145-8. eCollection 2018.
- Bettany-Saltikov J, Turnbull D, Ng SY, et al; Management of Spinal Deformities and Evidence of Treatment Effectiveness. Open Orthop J. 2017 Dec 29;11:1521-1547. doi: 10.2174/1874325001711011521. eCollection 2017.
- Ali A, Fontanari V, Fontana M, et al; Spinal Deformities and Advancement in Corrective Orthoses. Bioengineering (Basel). 2020 Dec 25;8(1):2. doi: 10.3390/bioengineering8010002.
- Smith JS, Shaffrey CI, Ames CP, et al; Treatment of adult thoracolumbar spinal deformity: past, present, and future. J Neurosurg Spine. 2019 May 1;30(5):551-567. doi: 10.3171/2019.1.SPINE181494.
Sobre o autorVer biografia completa

Dr Colin Tidy, MRCGP
Médico Generalista, Autor Médico
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy é um médico do NHS, baseado em Oxfordshire.
Sobre o revisorVer biografia completa

Dr Hayley Willacy, FRCGP
Médico Generalista, Autor Médico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
A Dra. Hayley Willacy era uma médica do NHS atuando no noroeste da Inglaterra, que se aposentou da prática clínica em 2022 após 30 anos.
Histórico do artigo
As informações nesta página são escritas e revisadas por clínicos qualificados.
Artigo também disponível em Inglês, Alemão, Espanhol, Francês, Italiano, Português, Hindi, Hebraico, Árabe, e Sueco.
Próxima revisão prevista: 14 Mar 2028
16 Mar 2023 | Última versão

Pergunte, compartilhe, conecte-se.
Navegue por discussões, faça perguntas e compartilhe experiências em centenas de tópicos de saúde.

Sentindo-se mal?
Avalie seus sintomas online gratuitamente
Inscreva-se no boletim informativo do Patient
Sua dose semanal de conselhos de saúde claros e confiáveis - escritos para ajudá-lo a se sentir informado, confiante e no controle.
Ao se inscrever, você aceita nossos Política de Privacidade. Você pode cancelar a inscrição a qualquer momento. Nunca vendemos seus dados.
Mais sobre ossos, articulações e músculos
- Espondilite anquilosante
- Espondiloartrite axial
- Bifosfonatos
- Costelas quebradas ou contusas
- Condrocalcinose
- Luxação
- Lesões e fraturas no antebraço
- Gânglio
- Lesão no tendão
- Substituição de quadril
- Dor nas articulações
- Dor lombar
- Esclerose múltipla
- Distrofia muscular
- Bursite do olecrano
- Osteomielite
- Prevenção da osteoporose induzida por esteroides
- Artrite psoriática
- Rabdomiossarcoma
- Cotovelo de tenista