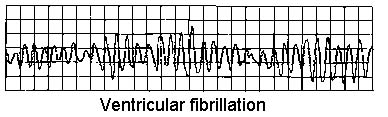
Fibrilação ventricular
Revisado por Dr Toni Hazell, MRCGPÚltima atualização por Dr Hayley Willacy, FRCGP Última atualização 23 de maio de 2023
Atende aos diretrizes editoriais
- BaixarBaixar
- Compartilhar
- Language
- Discussão
- Versão em Áudio
- Adicionar às fontes preferidas no Google
Profissionais de Saúde
Os artigos de Referência Profissional são projetados para uso por profissionais de saúde. Eles são escritos por médicos do Reino Unido e baseados em evidências de pesquisa, diretrizes do Reino Unido e da Europa. Você pode encontrar o Ritmos cardíacos anormais artigo mais útil, ou um dos nossos outros artigos de saúde.
What is ventricular fibrillation?
Ventricular fibrillation (VF) is a cause of cardiac arrest and sudden cardiac death. The ventricular muscle fibres contract randomly causing a complete failure of ventricular function. Most cases of ventricular fibrillation occur in patients with pre-existing known heart disease (with myocardial fibrosis - scarring - having a role1 ) but the precise nature of the underlying cause of VF is not currently known.
How common is ventricular fibrillation? (Epidemiology)
VF is the most commonly identified arrhythmia in cardiac arrest patients and has been reported as present in 70% of cardiac arrests.2
The incidence of VF parallels the incidence of ischaemic heart disease, with a peak incidence of VF occurring in people aged 45-75 years.
Fatores de risco
VF is most often associated with coronary artery disease and as a terminal event. VF may be due to acute myocardial infarction (MI) or ischaemia, or occur because of a chronic infarction scar.
When electrocardiogram documentation is available, it often shows that rapid VT precedes VF.
VF can occur during any of the following conditions or situations:
Antiarrhythmic drug administration.
Hipóxia.
Isquemia.
Very rapid ventricular rates in the pre-excitation syndrome.
Electrical shock administered during cardioversion.
Electrical shock caused by accidental contact with improperly grounded equipment.
Competitive ventricular pacing to terminate ventricular tachycardia (VT).
VF can occur in healthy, young athletes after a blunt (non-penetrating) blow to the chest.3 This known as commotio cordis.
Presentation of ventricular fibrillation
Patients may have a history of chest pain, fatigue, palpitations and other nonspecific complaints.
There may be known diagnosis or suggestion of pre-existing heart disease - eg, coronary artery disease, cardiomyopathy, valvular heart disease, miocardite, congenital heart disease, long QT syndrome, Wolff-Parkinson-White (WPW) syndrome or Brugada's syndrome.
Diagnóstico diferencial
Arrhythmias associated with cardiac arrest are divided into two groups:
Shockable rhythms: VF and VT.
Non-shockable rhythms: asystole and pulseless electrical activity (PEA): see the separate article on Adult Cardiopulmonary Arrest.
Other causes of sudden collapse such as dissecção aórtica e embolia pulmonar.
Investigações
VENTRICULAR FIBRILLATION
Enzimas cardíacas (troponin).
Electrolytes, calcium and magnesium. Severe metabolic acidosis, hypokalaemia, hyperkalaemia, hypocalcaemia, and hypomagnesaemia are some of the conditions that can increase the risk for arrhythmia and sudden death.
Drug levels (eg, tricyclic antidepressants, digoxin). Most of the anti-arrhythmic medications also have a pro-arrhythmic effect.
Toxicology screen: drugs that can lead to vasospasm-induced ischaemia - eg, cocaine.
Thyroid-stimulating hormone (TSH): hyperthyroidism can lead to tachycardia and tachyarrhythmias.
ECG:4 evidence of MI, prolonged QT interval, short PR, WPW pattern or other conditions.
Raio-X de tórax: signs of left heart failure, pulmonary hypertension.
Ecocardiografia: underlying structural abnormalities and cardiac dysfunction.
Nuclear imaging techniques:
Resting thallium (Tl) or technetium Tc 99m scintigraphy: assessing myocardial damage after MI.
Exercise nuclear scintigraphy: very sensitive in detecting the presence, extent and location of myocardial ischaemia.
Angiografia coronária:
Cardiac catheterisation in patients who survive VF, to assess the state of ventricular function and severity and extent of coronary artery disease.
Coronary angiography identifies patients who may benefit from revascularisation by percutaneous coronary intervention (angioplasty) or coronary artery bypass grafting (CABG), and can also help identify coronary artery anomalies and other forms of congenital heart disease.
Management of ventricular fibrillation2
See the separate articles on Adult Cardiopulmonary Arrest e Desfibrilação e Cardioversão. Early defibrillation is essential to improve outcome.
Medical stabilisation
Patients who survive the initial episode of VF require a full evaluation of left ventricular function, myocardial perfusion and electrophysiological stability.
Careful post-resuscitation care is essential to survival because recurrence rates average at about 50%.
Treatment of myocardial ischaemia, heart failure and electrolyte disturbances.
Empirical beta-blockers are often given.
Most survivors of VF should be treated with implantable cardioverter defibrillators (ICDs).5 Transvenous ICDs can be placed with minimal morbidity and mortality.
Radiofrequency ablation: most cases of VF are not amenable to radiofrequency ablation and require ICD placement.
By itself, CABG only prevents recurrent VF if the ejection fraction is normal and ischaemia was the cause of the arrest. Even in these patients, ICDs are frequently placed after CABG.
Complications of ventricular fibrillation
Central nervous system ischaemic injury.
Myocardial injury.
Post-defibrillation arrhythmias.
Defibrillation injury to self or others.
Injuries from CPR and resuscitation.
Skin burns.
Morte.
Prognóstico
Prognosis for survivors of VF strongly depends on the time elapsed between onset and medical intervention (prognosis is poor without intervention by 4-6 minutes after onset of VF) as well as on the particular aetiology for the VF.
Early defibrillation often makes the difference between long-term disability and functional recovery.6 If defibrillation is delivered promptly, survival rates as high as 75% have been reported.7
Death and disability after successful resuscitation correlate with the degree of central nervous system damage occurring during the event due to anoxia.
VF that occurs within the first 48 hours of the onset of acute MI has no bearing on prognosis, but VF that occurs more than 48 hours after acute MI is associated with a high rate of recurrence and a poorer prognosis.
After resuscitation, the prognosis is largely dependent on haemodynamic stability, early neurological recovery and duration of the resuscitation.
Education and training of non-healthcare professionals in basic life support and the use of automated external defibrillators in public places probably have the greatest impact on improving survival rates.
A major adverse outcome from a VF event is anoxic encephalopathy.
Atualizações exclusivas para profissionais de saúde
Mantenha-se informado com as últimas atualizações clínicas, insights profissionais e orientações baseadas em evidências. O boletim informativo Patient Pro seleciona conteúdo essencial para profissionais de saúde—entregue diretamente na sua caixa de entrada.
Ao se inscrever, você aceita nossos Política de Privacidade. Você pode cancelar a inscrição a qualquer momento. Nunca vendemos seus dados.
Leitura adicional e referências
- Adult Tachycardia Algorithm; Resuscitation Council (UK), 2015 (updated 2021).
- Bezzerides VJ, Pu WT; Two sides of the same coin: new insights into mechanisms of ventricular fibrillation. Cardiovasc Res. 2021 Mar 21;117(4):983-984. doi: 10.1093/cvr/cvaa246.
- Ludhwani D, Goyal A, Jagtap M; Ventricular Fibrillation.
- Patel N, Pena C, Nesheiwat Z, et al; Ventricular fibrillation arrest after blunt chest trauma in a 33-year-old man, commotio cordis? BMC Cardiovasc Disord. 2022 Jun 3;22(1):252. doi: 10.1186/s12872-022-02689-4.
- Biblioteca de ECG
- Desfibriladores cardioversores implantáveis e terapia de ressincronização cardíaca para arritmias e insuficiência cardíaca; Orientação de Avaliação de Tecnologia do NICE, junho de 2014
- Adgey AA, Spence MS, Walsh SJ; Theory and practice of defibrillation: (2) defibrillation for ventricular fibrillation. Heart. 2005 Jan;91(1):118
- Diretrizes de Suporte Avançado de Vida para Adultos 2021; Conselho de Ressuscitação do Reino Unido
Sobre o autorVer biografia completa

Dr Hayley Willacy, FRCGP
Médico Generalista, Autor Médico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
A Dra. Hayley Willacy era uma médica do NHS atuando no noroeste da Inglaterra, que se aposentou da prática clínica em 2022 após 30 anos.
Sobre o revisorVer biografia completa

Dra. Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
A Dra. Toni Hazell se formou na Escola de Medicina do Hospital St. Mary e fez seu VTS no Hospital Northwick Park.
Histórico do artigo
As informações nesta página são escritas e revisadas por clínicos qualificados.
Artigo também disponível em Inglês, Alemão, Espanhol, Francês, Italiano, Português, Hindi, Hebraico, Árabe, e Sueco.
Próxima revisão agendada: 21 de maio de 2028
23 de maio de 2023 | Última versão

Pergunte, compartilhe, conecte-se.
Navegue por discussões, faça perguntas e compartilhe experiências em centenas de tópicos de saúde.

Sentindo-se mal?
Avalie seus sintomas online gratuitamente
Mais sobre doenças cardiovasculares
- Terapia de ablação para arritmias
- Monitoramento ambulatorial da pressão arterial
- Aneurismas e dissecção de artérias
- Dissecção aórtica
- Pontuação CHA₂DS₂-VASc
- Vasoespasmo da artéria coronária
- Dor de cabeça
- Síndrome de Kartagener
- Marcapassos e estimulação
- Cuidados paliativos para insuficiência cardíaca
- Polimialgia reumática
- Hipertensão portal
- Cefaleia primária associada à atividade sexual
- Síndrome do nó sinusal doente
- Tromboflebite superficial
- Tratamento e gestão do diabetes tipo 2
- Defeito do septo ventricular
- Critérios de Wells para trombose venosa profunda (TVP)
- Síndrome de Wolff-Parkinson-White